Clearly, the COVID-19 pandemic poses significant challenges for doctors and hospitals. For example, there are major capacity management issues and it possibly very hard choices will have to be made whether to treat a patient or not with only limited prognostic parameters available.
At Holland AI, we have been contemplating various avenues to offer non-profit support. We have added new functionalities to our application for detection of pulmonary nodules, analyzing the extent of lung damage by COVID-19.The main opinion of our team was that we should not engage in developing COVID-19 solutions unless we had the feeling that we could add real value to the scientific work being done on the pandemic. Also, we explicitly don’t want to leverage this crisis for commercial stakes.
Several algorithm vendors have developed (or are developing) algorithms for detection of COVID-19 on chest-CT scans or X-ray images of the chest. These solutions can definitely add value in situations where there is scarcity of radiologists in combination with a high volume of CT-scans.
However, in the Netherlands scarcity of radiologists is – knock-on-wood – not a problem at this moment. In addition, CT-features of COVID-19 are highly aspecific and can also be found in, for example, other types of pneumonias, and it remains unclear if an AI-tool can distinguish pneumonias based on their causative pathogen.
So, where can we add value using AI in this situation? As mentioned before, treatment decisions must be made and there are only a few prognostic parameters available. Several studies have used the so-called CT-severity score to make an estimation of the affected lung tissue in each lung lobe. One can imagine that patients with only 5% affected tissue may have a better prognosis than a patient with 50% damage, presenting on the same day after the onset of complaints. Dutch radiologists are currently reporting this score in the standard COVID-19 reporting template. However, this is an additional task in the ever-growing list of radiologist’s tasks and time-consuming in terms of assessment and reporting.
In addition, the CT-severity output can be used for integration in predictive models using other input data (e.g. blood samples and clinical parameters). In this way, the CT-severity score can important value for doctors (e.g. ICU-doctors and pulmonologists) to decide on the follow-up of treatment.
Considering this, we have decided to tweak and adjust the advanced segmentation capabilities of PulmoFast (our in-house algorithm for detection of pulmonary nodules), and deploy a model to provide quantification of the CT-severity score. The first version of this solution was built in only one week and we are very grateful for the tremendous teamwork. Of course, this is the first version and we are currently fast-tracking a development study in one of our main partner institutions (Maasstad Ziekenhuis Rotterdam). We will offer an API solution for all hospitals in the EU to use this tool free of charge.
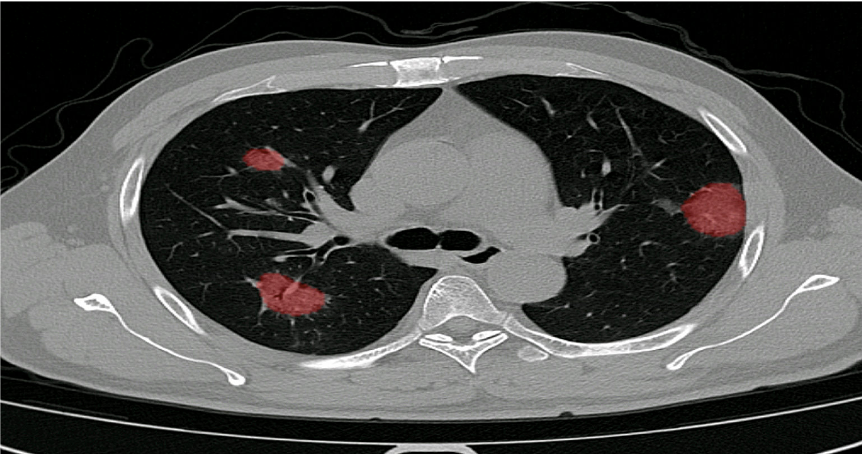
How it works:
Automated scoring of the extend of damage inflicted on the lung due to COVID-19.
Scoring is shown per individual lobe, consistent with the scores used in numerous clinical studies
Fully integrated into existing workflow and PACS viewer.
Why do we do this from a developer’s point of view? To prove ourselves that we can develop such a solution within 2 weeks, with easy implementation, in full compliance with all relevant law and legislation. And after the crisis, we are happy to talk about how we can help your institution during ‘normal’ times with improving healthcare by deploying AI and machine learning.